
Plan a consultation on Doctolib
Pioneer and leader in lymphoedema surgery
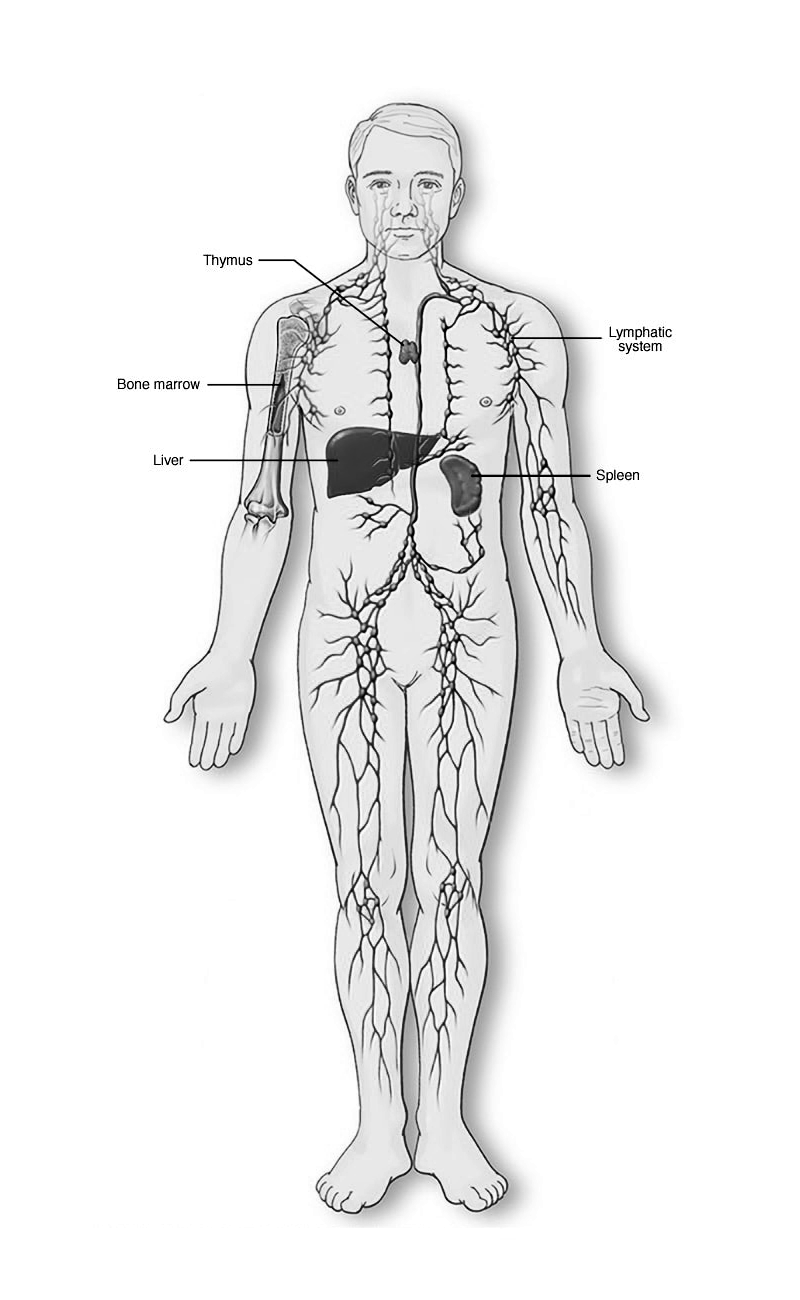
WHAT IS LYMPHOEDEMA?
Lymphoedema refers to tissue swelling caused by an accumulation of protein-rich fluid that's usually drained through the body's lymphatic system.
Symptoms include :
Swelling of part or all of the arm or leg, including fingers or toes
A feeling of heaviness or tightness
Restricted range of motion
Recurring infections
Hardening and thickening of the skin (fibrosis)
Lymphoedema can be primary, congenital or secondary, caused by f.e. cancer, cancer treatment, infection, trauma, parasites etc.
Both forms can be surgically treated.

FIELD OF EXPERTISE
CONGENITAL LYMPHOEDEMA
Lymphoedema is a pathologic condition that results from a disturbance of the lymphatic system, with localized fluid retention and tissue swelling. Swelling can affect a single limb, multiple limbs, genitalia or the face.
Primary lymphoedema is a congenital disorder, due to a malformation of lymph vessels and/or nodes (hypotrophic or hypertrophic).
Congenital lymphoedema can appear at birth or during the first years of the life. In most of the cases it develops during puberty, perhaps due to the hypotrophy of the lymphatic system which is too small for the growing body, or dysplasia.
Lipoedema is a congenital pathology and due to lymphatic disorders and has to be well evaluated multidisciplinary (micronutrition, resistance to insulin, hormonal status etc).
Diagnosis
The clinical aspect and the history are important.
Complementary investigations
Nowadays, radiological evaluation of lymphedema patients can be done through lymphoMRI.
PDE (Photodynamic eye) provides information on the superficial lymphatic network.
Magnetic Resonance Lymphography (MRL), with T3 weighted imaging, allows visualization of the lymphatic system anatomy with greater sensitivity than lymphoscintigraphy, without the need of any injection.
Surgical treatments
Lymphnodes transplantation:
The principle is to take some nodes with their own vessels in a place of the body where there are enough nodes and where there is no effect of the drainage of the donor site. The flap is inserted in the area where the nodes and the lymphatic vessels are insufficient and will survive thanks to micro anastomosis of the vessels under microscope.
The healthy nodes contain a growth hormone (VGEF 3) which induces neoformation of lymphatic ducts. They also help fighting again infections.
Lymphovenous anastomosis:
Rerouting of the lymphatic vessels in a mini vein, when the lymphatic pressure is too high and the lymphatic vessels have still a good quality.
Liposculpture:
Liposuction under the control of the fluoroscopy to avoid lymphatic damages, allows the removal of all the fat deposits.
Debulking:
In case of elephantiasis, resection of the excess of skin and folds can be mandatory.
IATROGENIC LYMPHOEDEMA
Secondary lymphoedemas are common in oncologic treatment, especially after lymph node dissection and radiotherapy. The drainage of the limb is totally interrupted.
Cancers, whose treatments are commonly associated with lymphoedema, include pelvic tumors (i.e., enlarged hysterectomies and prostatectomies), Hodgkin’s tumors, sarcoma and melanoma and cancers of the breast for the upper extremity.
Alternatively, lymphoedema may also be caused by non-oncologic procedures such as saphenous vein removal, hernia repair, or thigh lifts, internal liposuctions.
The lymphoedema can appear immediately or many years after the surgery. Chronic infections can destroy all the remaining lymphatic collectors and elephantiasis can occur with skin thickening, folds, redness, fibrosis.
Diagnosis
The diagnosis is made by clinical exam, isotopy and lymphoMRI.
Surgical treatments
Reconstruction of the damaged area (by the removal of the nodes and the radiotherapy) can be done after resection of the fibrotic tissue covering this region with a fatty free flap containing nodes. This flap is reconnected by microsurgery.
In case of mastectomy, the breast can be rebuilt with a free flap (DIEP), pediculated flap (dorsalis) or with a prothesis, and the lymphatic flap can be anastomosed to some vessels in the axillary region.
In case of treatment for cancer of the uterus, prostate, or melanoma, the reconstruction of the deep lymphatic system by this free lymphatic flap is performed.
Liposculpture allows the removal of the excess fat accumulation during those lymphoedema years.
Lymphovenous anastomoses (shunts between lymphatic vessels and veins) are appropriate in mild cases, mostly distally.
Debulking can be necessary in elephantiasis cases.
LIPOEDEMA
Some patients, even if they are thin, have big legs with swollen ankles since the puberty and experience pain.
The evaluation is very important, because the normal liposuction can not treat at all, and can even worsen the situation: the canula can destroy the few present lymphatic vessels. In cases of combination of lymphoedema and lipoedema, the lymphnode transplantation can really help and maintain the results over the time in mild lymphoedema, lymphovenous anastomosis at the ankle can really help.
LYMPHOEDEMA IN CHILDREN
Can be severe, and multilocalisations are to be evaluated.
Pluridisciplinary approach is mandatory, but also very promising.
In hypoplastic cases, lymph nodes transplants can cure them.




ABOUT
Dr. Corinne Becker is a plastic surgeon trained in Belgium, France, Germany with the best professors in plastic and hand surgery. She dedicated her life to treating patients suffering from lymphoedema and invented the procedure of the lymph nodes transplantation to treat this disease. She combines different techniques and substantially improves the long term surgery results of the lymphoedema and lipoedema patients.
With more than 25 years of experience in lymphoedema treatment, on more than 5000 patients, she can substantially improve the quality of life of many patients. With high chance of being completely cured by the treatment.
In her career, she also trained for four years with the plastic surgery team of B. Allen to develop the lymphatic surgery in New York at the Ear and Eye Infirmary Hospital (NYEE), New York University (NYU).
Dr. Becker now works in Paris, at Ambroise Paré Clinic and Clinical Bizet.
She is a member of the French Academy of Surgery, an invited professor at NYU and Stanford university, in Argentina, Vietnam and Italy.
Dr. Becker participates in various international conferences and operates all around the world.